

The menisci are crescent-shaped fibrocartilaginous structures within the knee joint that play crucial roles in load distribution, shock absorption, joint stability, and cartilage nutrition. Their unique macro- and micro-structure, including circumferential and radial collagen fiber orientations, enables them to convert compressive forces into hoop stresses, preserving knee joint integrity.
Meniscal injuries are common, particularly in physically active populations and pediatric patients, and can result from acute trauma or degenerative changes. Different types of meniscal tears include:
- Vertical longitudinal tears: Typically occur in the vascular peripheral zones and have the best healing potential.
- Radial tears: Disrupt circumferential fibers and hoop stresses, often requiring more conservative management.
- Horizontal tears
- Bucket-handle tears
- Complex tears
- Root tears: Disruption of the meniscal root attachment, often requiring more protective postoperative rehabilitation.
Each tear type presents unique biomechanical challenges and healing potentials, which influence surgical repair techniques and postoperative rehabilitation protocols. Rehabilitation must be tailored to tear type, repair method, and patient factors to optimize healing and functional outcomes.
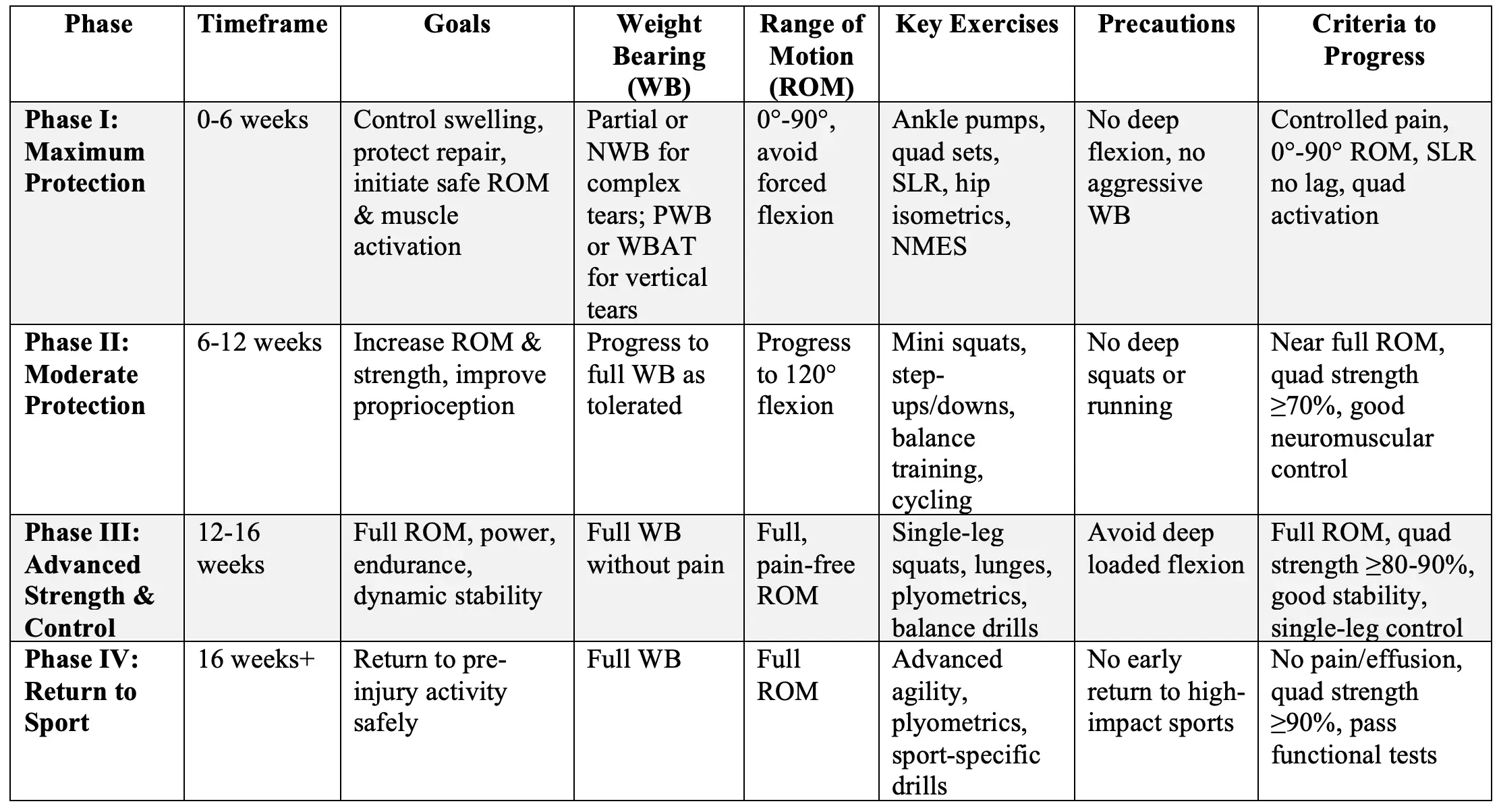
Phase-Based Rehabilitation Protocol
Phase I: Maximum Protection (Weeks 0-6)
Goals:
- Control inflammation and swelling
- Protect the meniscal repair site
- Begin safe restoration of range of motion (ROM)
- Initiate muscle activation, especially quadriceps
- Maintain cardiovascular fitness (as tolerated)
Interventions:
- Cryotherapy and elevation to reduce pain and swelling
- Use of knee brace locked in extension (0°) for protection (duration varies by tear type)
- Weight bearing (WB) status varies by tear type (see notes below)
- Controlled passive and active-assisted ROM exercises within prescribed limits
- Neuromuscular electrical stimulation (NMES) to quadriceps when indicated
- Isometric quadriceps activation
- Hip and core muscle isometrics
- Patellar mobilizations- all directions
- Balance/proprioception and neuromuscular control (e.g., weight shifting, double-limb balance exercise)
- Blood Flow Restriction (BFR) training when appropriate (screen for contraindications)
Exercise List:
- Ankle pumps for circulation
- Quadriceps sets and isometrics
- Straight leg raises (SLR) without lag
- Passive knee extension with support
- Hip abduction/adduction isometrics
- Core stabilization (planks)
- Controlled passive ROM: 0° to 90° as tolerated (varies with tear)
- Prone terminal knee extension
- Weigh shifting in allowed range
Precautions and Risks:
- Avoid forced knee flexion beyond prescribed limits (usually 90°)
- Avoid weight bearing beyond prescribed status to prevent repair failure
- Avoid hamstring strengthening if posterior horn repair until cleared
- Avoid deep squatting, pivoting, and rotational movements
- Avoid flex CKC exercises beyond 60°
Weight Bearing & ROM Notes:
- Vertical longitudinal tears: Partial WB as tolerated immediately or within first 2 weeks; ROM limited to 0-90°
- Radial, complex, root tears: Non-weight bearing (NWB) or toe-touch WB (TTWB) for 4-6 weeks; ROM restricted to 0-90°
- Immobilization: Use of brace locked in extension for 2-6 weeks depending on tear complexity
Criteria to Progress to Phase II:
- Controlled pain and minimal swelling/effusion
- Achieve 0° to 90° passive ROM
- Ability to perform SLR without quadriceps lag
- Adequate quadriceps activation (MMT 4/5 or better)
- Safe and controlled weight bearing within prescribed limits
Phase II: Moderate Protection / Strengthening (Weeks 6-12)
Goals:
- Increase knee ROM towards full range (usually aiming for full extension and flexion >110°)
- Improve quadriceps and lower extremity strength
- Enhance neuromuscular control and proprioception
- Begin low-impact aerobic conditioning
Interventions:
- Continue effusion management strategies
- Progress from isometric to isotonic strengthening of quadriceps, hamstrings, hip musculature
- Closed kinetic chain (CKC) exercises emphasizing joint stability
- Progress proprioceptive neuromuscular training (balance exercises on stable and unstable surfaces)
- Gradual increase in weight bearing to full WB as tolerated
- Gradual increase in knee flexion ROM (targeting 120° by 12 weeks)
- Aquatic therapy and stationary cycling with low resistance
- Continue BFR if tolerated
Exercise List:
- Mini squats (0-45° flexion)
- Step-ups and step-downs
- Single-leg stance and balance exercises with eyes open/closed
- Hamstring curls with resistance bands (starting week 6, except when restricted for posterior horn repairs)
- Gluteal bridges progressing to single leg bridges
- Core strengthening (planks, abdominal isometrics)
- Low resistance cycling
Precautions and Risks:
- Avoid deep squatting (>90°) and running/jumping activities
- Monitor for swelling or increased pain; reduce intensity if present
- Avoid rotational stresses on the knee
Weight Bearing & ROM Notes:
- Full WB is generally allowed by 6 weeks for vertical tears; delayed for complex tears
- ROM should be progressively increased but typically limited to 120° by week 12
- Brace use may be discontinued based on clinical judgment
Criteria to Progress to Phase III:
- Near full, pain-free ROM (>110-120° flexion)
- Quadriceps strength ≥70% contralateral limb
- Good neuromuscular control demonstrated on single-leg balance and dynamic tasks
- No significant joint effusion or pain with functional activities
Phase III: Advanced Strength and Control (Weeks 12-16)
Goals:
- Achieve full, pain-free ROM
- Restore muscular strength, power, and endurance
- Improve dynamic knee stability and proprioception
- Begin controlled aerobic and low-impact plyometric activities
Interventions:
- Progress isotonic strengthening with increased resistance
- Begin plyometric exercises with emphasis on control
- Continue proprioceptive training on unstable surfaces
- Perturbation training and dynamic balance progression
- Initiate running progression on flat terrain
- Sport-specific drills at low intensity
- Cardiovascular conditioning (e.g., swimming, elliptical)
Exercise List:
- Step-ups/downs with increased height
- Single-leg calf raises
- Single-leg squats (progressing to 70-90° flexion)
- Lunges and lateral step-ups
- Plyometric drills (agility jumping, hopping)
- Balance board exercises and ball toss on unstable surfaces
- Low intensity jogging progressing to running
Precautions and Risks:
- Avoid deep loaded flexion, deep squatting, and twisting for at least 4 months
- Monitor for symptoms of instability or swelling
- Avoid high-impact activities until criteria met
Weight Bearing & ROM Notes:
- Full WB should be tolerated without pain
- Deep knee flexion and squatting allowed progressively after 3-4 months
- Return to running typically begins around 3-4 months
Criteria to Progress to Phase IV:
- Full, pain-free ROM
- Quadriceps strength ≥80-90% of contralateral limb
- Demonstrate good dynamic stability and neuromuscular control during functional tasks
- Ability to perform single-leg squats and hop tests with control
Phase IV: Return to Activity / Sports (Weeks 16 and Beyond)
Goals:
- Return to pre-injury level of activity and sports safely
- Maximize strength, power, endurance, and neuromuscular control
- Prevent re-injury through sport-specific training
Interventions:
- Advanced plyometric and agility training
- Sport-specific drills including cutting, pivoting, and jumping
- Continued strength training emphasizing power and endurance
- Cardiovascular conditioning tailored to sport demands
Exercise List:
- Agility and shuttle runs
- Single-leg hop for distance and timed hop
- Cutting and pivoting drills
- Plyometric exercises such as tuck jumps, box hops
- Core and hip stabilizer strengthening
- Lateral and multidirectional hopping drills
Precautions and Risks:
- Return to sport only after meeting objective criteria (see below)
- Avoid premature return to high-impact activities to minimize risk of re-tear
- Monitor for any signs of pain, swelling, or instability
Return to Sport Criteria:
- No knee pain or effusion
- Full knee ROM
- Quadriceps strength ≥90% compared to contralateral limb
- Successful completion of functional tests (e.g., hop tests) with ≥90% limb symmetry
- Adequate neuromuscular control and proprioception
Notes:
- Return to sport typically advised between 3-6 months post-op for vertical tears; may be delayed up to 9-12 months for complex or root tears
- Pediatric patients may require more cautious progression due to higher re-injury risk with early return
Additional Considerations
- Functional Testing: Functional tests such as single-leg hop tests can help identify patients who need additional therapy before return to sports. Most isolated meniscal repair patients achieve acceptable limb symmetry by 4 months post-op, similar to ACL reconstruction patients at 6 months
- Immobilization: Prolonged immobilization may negatively affect meniscal healing by reducing vascular supply. Early controlled mobilization and weight-bearing have been shown to be safe and beneficial for certain tear types
- Rehabilitation Variation: There is significant heterogeneity in rehabilitation protocols worldwide. No single protocol has demonstrated superiority, emphasizing the need for individualized, criterion-based progression
- Return to Sport: Most studies suggest return to sport between 3-6 months post meniscal repair, with longer times for complex tears. Objective criteria-based decision-making reduces risk of re-injury
- Neuromuscular Training and Myofascial Release: Early incorporation of proprioceptive neuromuscular training and myofascial release techniques may improve pain, function, and neuromuscular control
Common Patient Questions and Answers
When can I start putting weight on my leg after meniscus repair?
For many types of meniscus tears, especially vertical longitudinal tears, early weight bearing as tolerated is safe and does not increase the risk of repair failure. However, your surgeon will tailor this based on your specific tear and surgery.
How much knee bending (flexion) am I allowed after surgery?
Typically, knee bending is limited initially to 30-90 degrees depending on tear type, then gradually increased over 4-6 weeks. Deep bending and twisting movements are avoided for at least 3-4 months.
When can I return to sports?
Return to sports is usually allowed between 3 to 6 months post-surgery after meeting specific criteria such as pain-free full range of motion, adequate muscle strength (at least 80-90% of the other leg), and good neuromuscular control.
Will I need a knee brace during rehab?
Use of a knee brace depends on the type of tear and the surgeon’s preference. It may be used locked in extension for the first few weeks to protect the repair, but is typically discontinued by 6 weeks.
What happens if my meniscus repair fails?
If the repair fails, you may require further surgery such as partial meniscectomy. Studies show that failure negatively impacts knee function and quality of life.
Reference:
- Harput, G., Guney-Deniz, H., Nyland, J., & Kocabey, Y. (2020). Postoperative rehabilitation and outcomes following arthroscopic isolated meniscus repairs: A systematic review. Physical Therapy in Sport, 45, 76-85. https://doi.org/10.1016/j.ptsp.2020.06.011
- Lucas, G., Accadbled, F., Violas, P., Sales de Gauzy, J., & Knörr, J. (2015). Isolated meniscal injuries in paediatric patients: Outcomes after arthroscopic repair. Orthopaedics & Traumatology: Surgery & Research, 101(3), 173-177. https://doi.org/10.1016/j.otsr.2014.12.006
- Mahadevan, R. D., Jayaprakasan, P., Shanker, P., & Irudhayaraj, L. (2023). The efficacy of early proprioceptive neuromuscular training and myofascial release technique following arthroscopic medial meniscal repair, a pilot study. International Journal of Academic Medicine and Pharmacy, 5(3), 645-652. https://doi.org/10.47009/jamp.2023.5.3.135
- Spang III, R. C., Nasr, M. C., Mohamadi, A., DeAngelis, J. P., Nazarian, A., & Ramappa, A. J. (2018). Rehabilitation following meniscal repair: a systematic review. BMJ Open Sport & Exercise Medicine, 4(1), e000212. https://doi.org/10.1136/bmjsem-2016-000212
- Kim, J. S., Lee, M. K., Choi, M. Y., Kong, D. H., Ha, J. K., Kim, J. G., et al. (2023). Rehabilitation after repair of medial meniscus posterior root tears: a systematic review of the literature. Clinics in Orthopedic Surgery, 15(5), 740-751. https://doi.org/10.4055/cios21231
- Lind, M., Nielsen, T., Faunø, P., Lund, B., & Christiansen, S. E. (2013). Free rehabilitation is safe after isolated meniscus repair: a prospective randomized trial comparing free with restricted rehabilitation regimens. American Journal of Sports Medicine, 41(12), 2753-2758. https://doi.org/10.1177/0363546513505079
- Perkins, B., Gronbeck, K. R., Yue, R. A., & Tompkins, M. A. (2017). Similar failure rate in immediate post-operative weight bearing versus protected weight bearing following meniscal repair on peripheral, vertical meniscal tears. Knee Surgery, Sports Traumatology, Arthroscopy. https://doi.org/10.1007/s00167-017-4665-9
- Pujol, N., Giordano, A. O., Wong, S. E., Beaufils, P., Monllau, J. C., Arhos, E. K., et al. (2025). The formal EU-US meniscus rehabilitation 2024 consensus: An ESSKA-AOSSM-AASPT initiative: Part I—Rehabilitation management after meniscus surgery (meniscectomy, repair and reconstruction). JOSPT Open, 3(3), 214-222. https://doi.org/10.2519/josptopen.2025.0162
- Grant, J. A., Wilde, J., Miller, B. S., & Bedi, A. (2012). Comparison of inside-out and all-inside techniques for the repair of isolated meniscal tears: a systematic review. American Journal of Sports Medicine, 40(2), 459-468. https://doi.org/10.1177/0363546511432540
- Becker, R., Wirz, D., Wolf, C., Gopfert, B., Nebelung, W., & Friederich, N. (2005). Measurement of meniscofemoral contact pressure after repair of bucket-handle tears with biodegradable implants. Archives of Orthopaedic and Trauma Surgery, 125(4), 254-260. https://doi.org/10.1007/s00402-005-0007-x
- Albrecht-Olsen, P., Kristensen, G., & Tormala, P. (1993). Meniscus bucket-handle fixation with an absorbable Biofix tack: development of a new technique. Knee Surgery, Sports Traumatology, Arthroscopy, 1(2), 104-106. https://doi.org/10.1007/BF01552601
- Stein, T., Mehling, A. P., Welsch, F., von Eisenhart-Rothe, R., & Jäger, A. (2010). Long-term outcome after arthroscopic meniscal repair versus arthroscopic partial meniscectomy for traumatic meniscal tears. American Journal of Sports Medicine, 38(8), 1542-1548. https://doi.org/10.1177/0363546510367516


