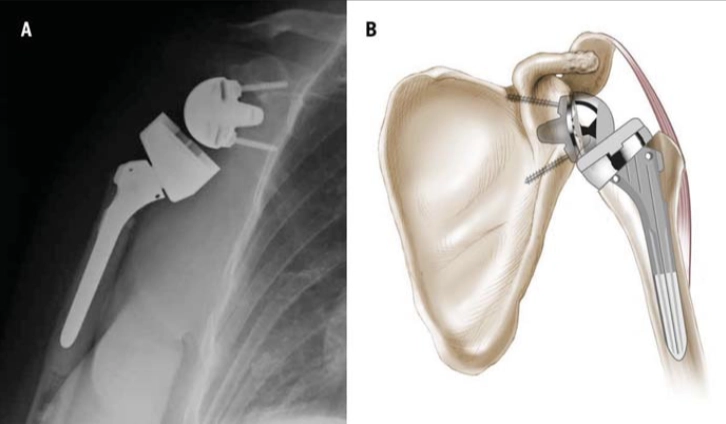
Photo adapted from Boudreau et al., 2007
Phase I: Immediate Post-Surgical / Joint Protection Phase (Day 1 to Week 6)
Goals:
- Protect the surgical repair and ensure healing of soft tissues.
- Maintain joint integrity.
- Control pain and inflammation.
- Maintain mobility and function of distal joints (elbow, wrist, hand).
- Begin gentle passive range of motion (PROM) within safe limits.
Precautions:
- Wear an abduction sling for comfort and protection (typically 4-6 weeks); can be discontinued earlier based on surgeon’s advice and patient tolerance. For the first 2-3 weeks post-operatively, the sling is typically worn full-time and removed only for hygiene, gentle exercises, and therapy sessions, in accordance with the surgeon’s recommendations.
- Avoid shoulder extension and IR beyond neutral.
- No active shoulder range of motion (AROM).
- Only light, NWB isometrics of scapular stabilizers and deltoid
- No lifting or weightbearing through the operated arm.
- Avoid combined shoulder internal rotation (IR), adduction, and extension (e.g., no reaching behind back or pushing from a chair) for at least the first 6 weeks.
- Protect the subscapularis repair if present; if repaired via superior approach, delay PROM and deltoid isometrics for 3-4 weeks.
Interventions:
- Cryotherapy for pain and swelling control.
- PROM of shoulder in scapular plane: forward flexion and external rotation gradually increased up to 90° and 20-30° respectively, avoiding abduction initially.
- Active and active-assisted ROM (AAROM) of elbow, wrist, and hand.
- Submaximal, pain-free deltoid and periscapular isometrics starting around day 4-7 (avoiding shoulder extension during posterior deltoid activation).
- Pendulum exercises.
- Patient and caregiver education on joint protection and safe movement.
List of Exercises:
- Pendulum exercises.
- Passive forward flexion and external rotation in scapular plane (in supine).
- Active elbow/wrist/hand movements.
- Submaximal deltoid isometrics (without shoulder extension).
- Scapular isometrics.
Criteria to Progress to Phase II:
- Patient tolerates PROM and AROM program for elbow, wrist, and hand.
- Ability to isometrically activate all deltoid components and periscapular muscles without pain.
- No signs of instability or complications.
Phase II: Active Range of Motion (AROM) and Early Strengthening Phase (Weeks 6 to 12)
Goals:
- Gradually restore active shoulder ROM.
- Re-establish dynamic shoulder stability.
- Begin gentle strengthening exercises.
- Submaximal isometric exercises (NWB only)
- Continue pain and inflammation control.
- Maintain joint protection.
Precautions:
- Continue avoiding shoulder hyperextension.
- Restrict lifting heavier than a coffee cup.
- Avoid weightbearing with the operative arm.
- If subscapularis repair was done, limit ER and IR as per surgeon’s instructions.
- Avoid sudden or jerky movements to minimize risk of dislocation
Interventions:
- Progress PROM to AAROM and then AROM in scapular plane (supine progressing to sitting/standing).
- Initiate gentle submaximal isometric external and internal rotation.
- Begin gentle isotonic strengthening of deltoid and periscapular muscles with low load, high repetition.
- Gentle scapulothoracic rhythmic stabilization and alternating isometric exercises.
- Continue cryotherapy as needed.
- Functional activities such as feeding and light ADLs encouraged.
- Restricted lifting with operated arm for 12-16 weeks (no more than a cup of coffee or glass of water)
- Delay resisted rotation to protect subscapularis and teres minor
List of Exercises:
- Pulley-assisted forward flexion.
- Assisted wall slides.
- Active forward flexion (gravity minimized progressing to upright).
- Submaximal ER strengthening in 45° to 90° abduction.
- Isometric deltoid and scapular stabilizer contractions.
- Gentle scapular retractions and protractions.
- Elbow, wrist, and hand strengthening.
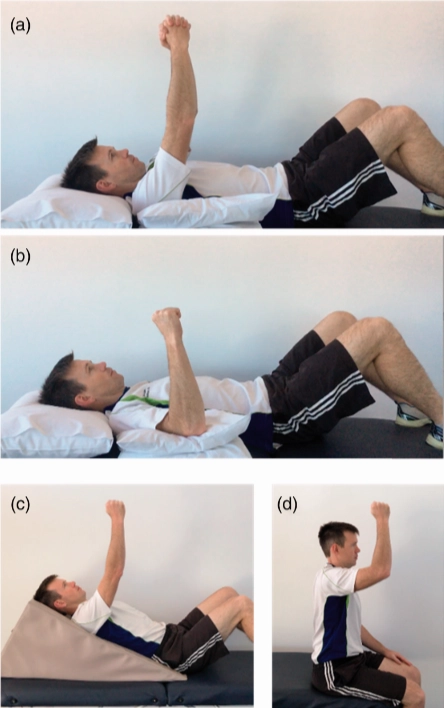
Progressive active forward flexion exercises, starting
with (a) supine ‘pray and lift’; (b) supine forward flexion; (c)
incline forward flexion; (d) upright forward flexion
Photo adapted from Edwards et al., 2021
Criteria to Progress to Phase III:
- Demonstrated improved shoulder function.
- Ability to isotonically activate all deltoid and periscapular muscles.
- Pain-free AROM with acceptable mechanics.
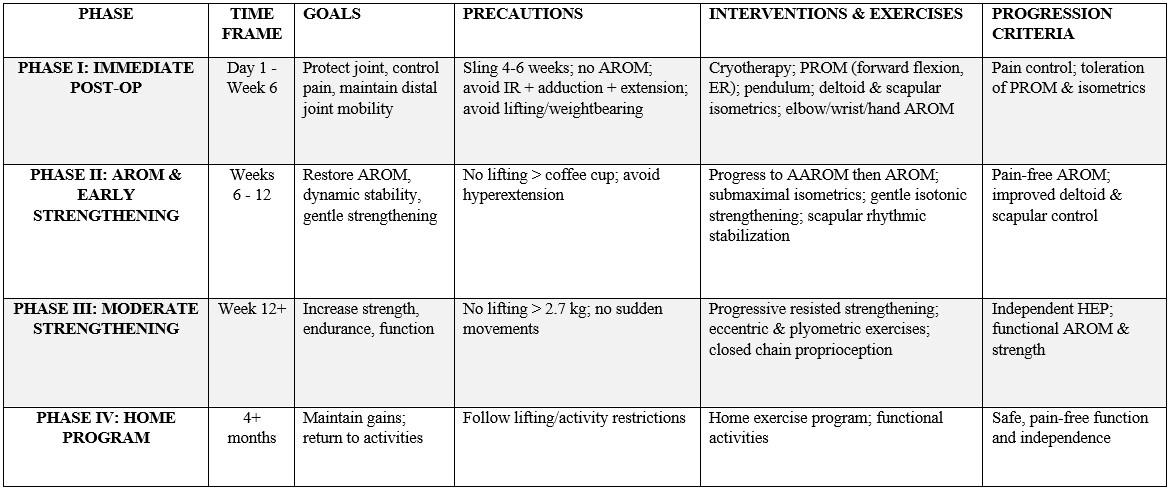
Summary Table of Rehabilitation Protocol