Proximal humerus fractures (PHFs), including humeral head fractures, are common injuries, particularly in elderly populations, often resulting from low-energy trauma such as falls. Management strategies vary depending on fracture complexity, patient age, bone quality, and functional demands. While many minimally displaced fractures are treated nonoperatively, complex and displaced fractures frequently require surgical intervention, most commonly open reduction and internal fixation (ORIF) with locking plates, intramedullary nailing (IMN), or shoulder arthroplasty.
Operative fixation aims to restore anatomy and provide stability to allow early mobilization, which is critical to prevent complications such as stiffness, frozen shoulder, and muscle atrophy. Postoperative rehabilitation is a vital component influencing functional outcomes. However, there is considerable variation in rehabilitation protocols, including immobilization duration, timing of passive and active range of motion (ROM) exercises, weight-bearing restrictions, and use of manual therapies. Different type of surgical fixation is also one of the key components of decision making for rehab plan.
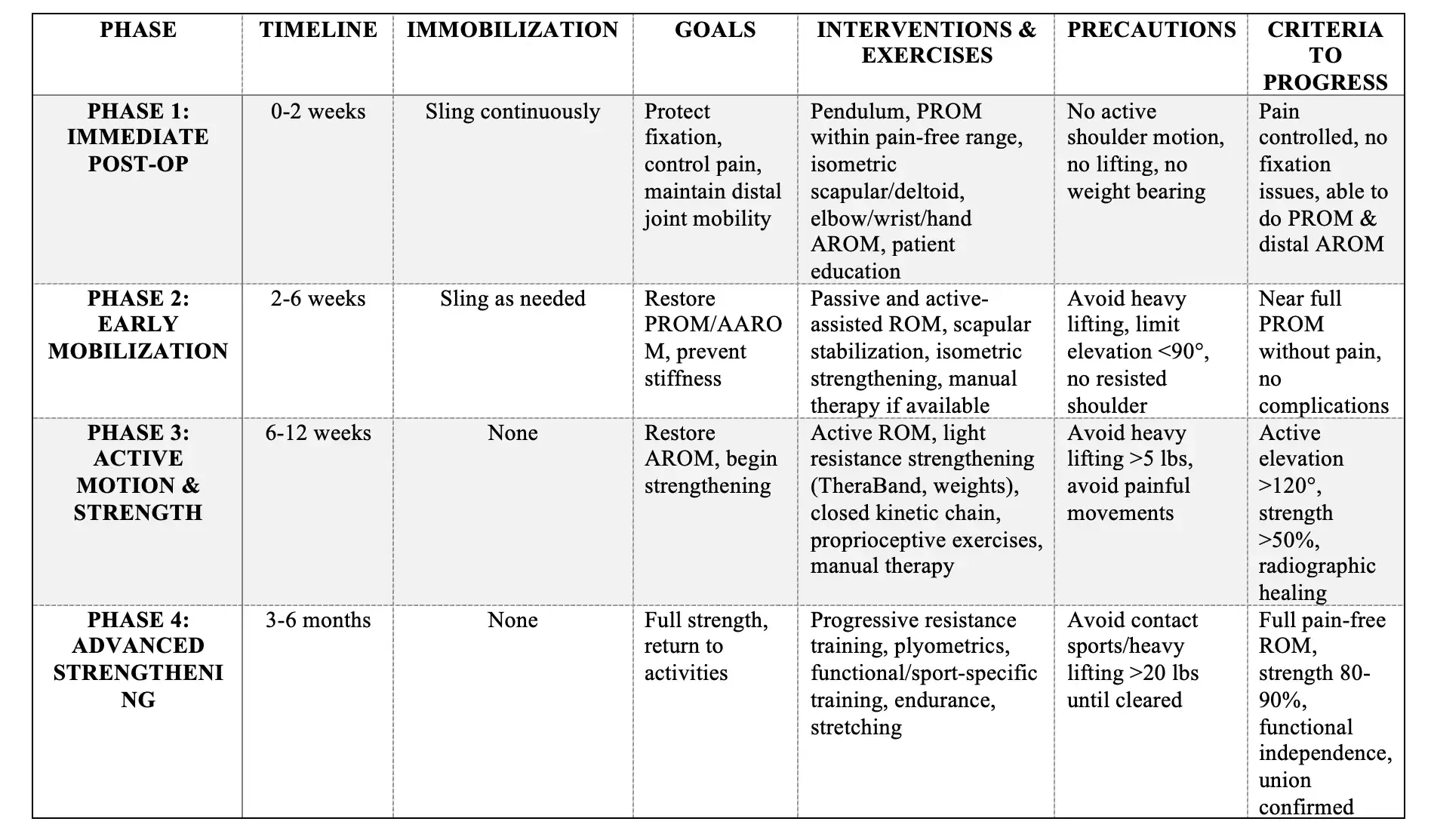
This protocol synthesizes current evidence and expert consensus to guide clinicians through an evidence-informed, phase-wise rehabilitation program following operative management of proximal humerus fractures.