Overview
Hip fractures are more common in older adults and occur at different rates around the world. In the United States, they are more common in women than men and are expected to increase as the population ages. Most hip fractures in people over 65 happen after a simple fall and are often related to weaker bones (fragility fractures). Although hip fracture rates have declined in some high-income countries due to improved osteoporosis management and fall prevention, rates continue to rise among the very elderly and in low- and middle-income populations.
These fractures are commonly classified as intracapsular or extracapsular. Intracapsular fractures involve the femoral neck, while extracapsular fractures include intertrochanteric and subtrochanteric fractures that occur around or just below the greater trochanter. Surgical management depends on the fracture type and patient-specific factors. Intracapsular fractures may be treated with internal fixation when stable or with hemiarthroplasty or total hip arthroplasty when displaced, with total hip arthroplasty often preferred in younger, more active patients. Extracapsular fractures are typically managed with internal fixation, most commonly using cephalomedullary nails or sliding hip screws, with cephalomedullary nails favored for unstable fracture patterns.
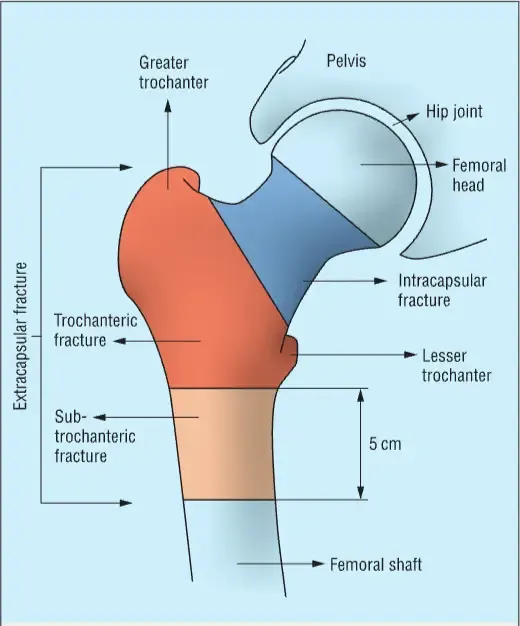
Photo Adapted from McDonough et al. (2021).
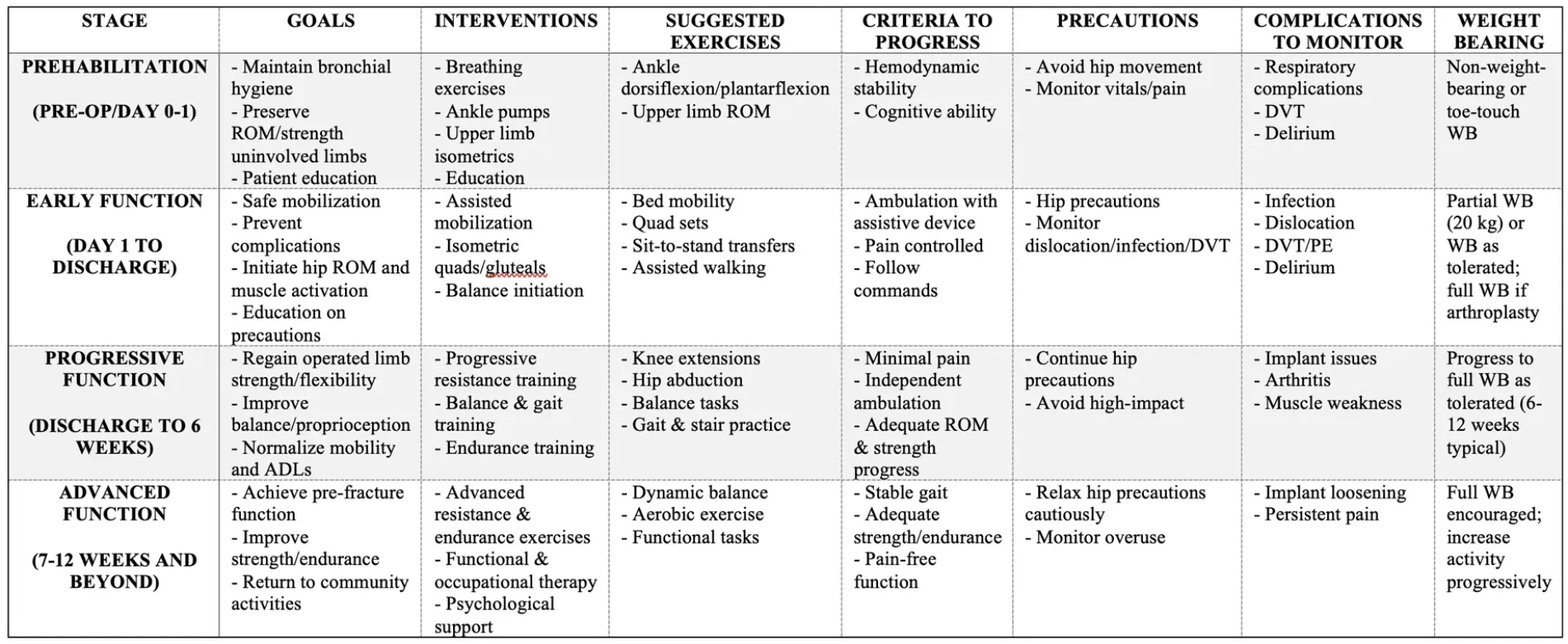
Summary Table of Postoperative Rehabilitation Protocol for Hip Fracture