Stage 1: Immediate Postoperative Phase (Day 0 to Day 3)
Goals
- Control pain and inflammation
- Prevent complications (e.g., deep vein thrombosis, infection)
- Initiate early mobilization and functional activities (sitting, standing, walking with aids)
- Restore knee range of motion (ROM) gradually
- Begin muscle activation, especially quadriceps
Precautions
- Monitor pain levels closely; keep pain manageable (NRS scores below 4 recommended)
- Avoid excessive swelling; control edema with proper positioning and cryotherapy
- Observe for signs of complications (dizziness, orthostatic hypotension, wound issues)
- Avoid unsupported walking and high-risk activities until sufficient strength and control are achieved
- Use assistive devices as recommended
Interventions
- Continuous Passive Motion (CPM) can be used briefly (~1 hour/day) within the first 24 hours but is not recommended as standard care due to lack of evidence for long-term benefits.
- Cryotherapy application to reduce pain and swelling; educate patient and caregivers on safe use.
- Compression bandaging and suction drainage management.
- Early mobilization: sitting, active ankle pumps, isometric quadriceps and gluteal sets, active-assisted knee flexion/extension within pain tolerance.
- Assisted standing and walking with walker or crutches initiated by Day 2-3.
- Patient education on safe transfers, use of assistive devices, and fall prevention.
Exercises
- Ankle pumps (to prevent venous stasis)
- Quadriceps setting (isometric contraction with knee extended)
- Gluteal sets
- Heel slides (active-assisted knee flexion)
- Assisted knee extension
- Bed mobility exercises (rolling, scooting, supine to sitting)
- Sit to stand with assistance
- Gait training with assistive devices
Important Points
- Early rehabilitation within 24 hours shortens hospital stay and improves outcomes.
- Pain control is essential to facilitate participation in therapy.
- Knee positioning during rest in mild flexion (30°-90°) can reduce postoperative swelling and blood loss without compromising long-term ROM.
- Monitor for and manage adverse effects such as dizziness and orthostatic hypotension.

Continuous Passive Motion (CPM) to restore knee Range of Motion
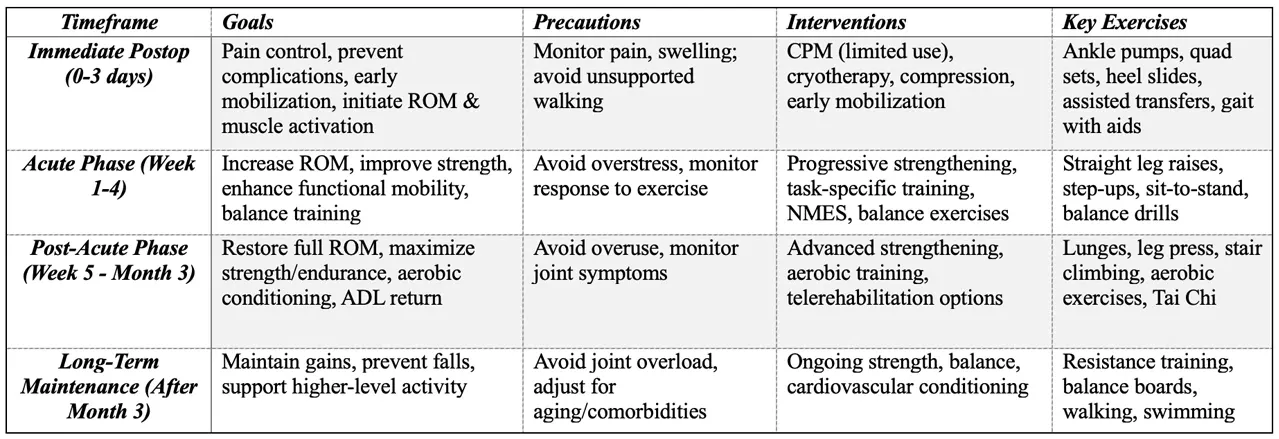
Summary Table of TKR Rehabilitation Protocol by Timeline