Phase 1: Acute Phase (Week 1)
Goal:
- Provide immobilization for pain relief and fracture stability.
- Minimize swelling and prevent stiffness in adjacent joints.
- Educate patient on injury and rehabilitation expectations.
Interventions:
- Immobilize the shoulder using an arm sling or a Gilchrist bandage, ensuring comfort and avoiding excessive tightness to prevent neurovascular compromise.
- Encourage active movement of fingers, wrist, and elbow to maintain mobility and circulation.
- Patient education on safe movements, pain management, and positioning (e.g., semi-reclined position for sleeping).
- Use of an axillary roll or pillow to counteract medial displacement forces from the pectoralis major muscle may be considered.
Immobilization:
- Arm sling or Gilchrist bandage; consider plaster reinforcement for unstable fractures.
- Immobilization in slight external rotation may reduce tuberosity displacement.
- Depending on the type of fracture and degree of deformity, different forms of immobilization may be required for the patient’s arm. Please refer to the examples below.
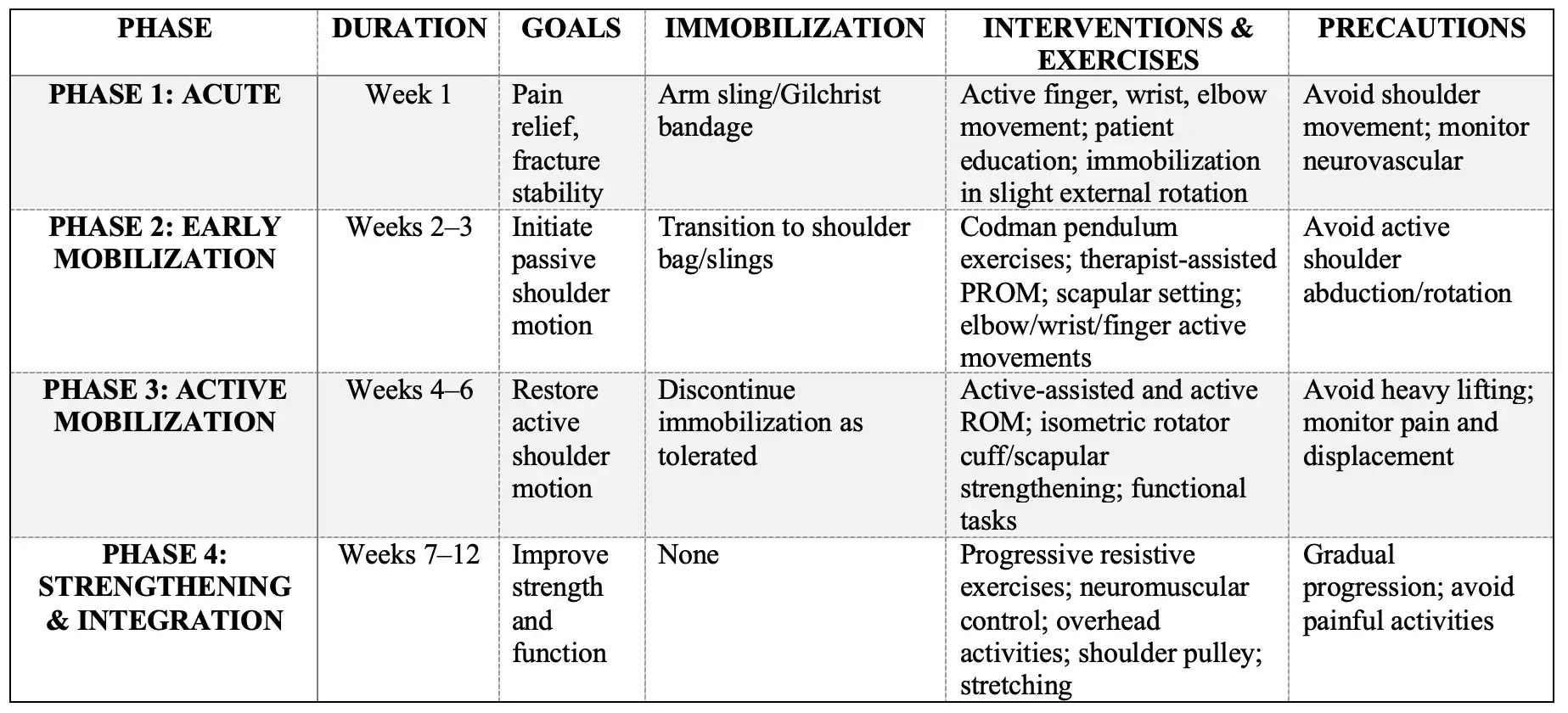
Simple Fracture: Patient with an arm sling. In this commercially available version, the upper arm and forearm are free and not encircled by the bandage as would be the case with the classic Gilchrist bandage (Razaeian et al., 2022)
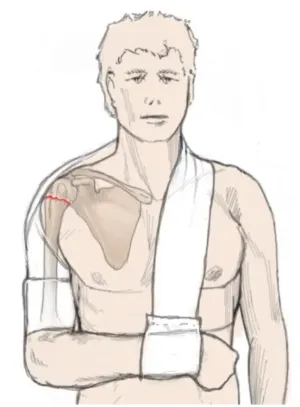
Varus-displaced fractures and/or greater tuberosity involvement: Patient with varus dis-placed fracture before (left) and after (right) application of the abduction orthosis. In this example, the humeral shaft is adjusted to the displaced humeral head fragment by abduction of the arm (Razaeian et al., 2022)
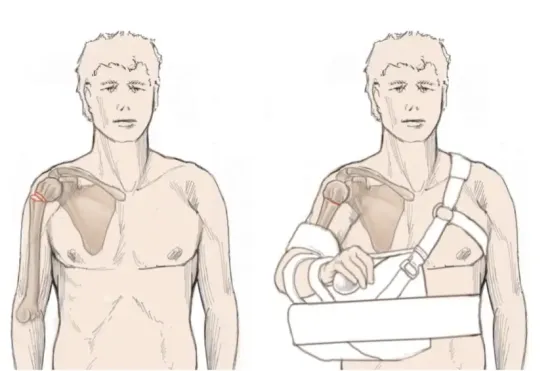
Counteract medial displacement: Patient with medial shaft translation before (left) and after (right) application of a Gilchrist bandage and axillary roll (Razaeian et al., 2022)
Precautions:
- Avoid active shoulder movements that could compromise fracture stability.
- Monitor for signs of neurovascular compromise or excessive swelling.
- Immobilization should not exceed 3-4 weeks to reduce risk of stiffness.
Exercise Examples:
- Active finger flexion and extension.
- Wrist circles and flexion/extension.
- Elbow flexion and extension within pain tolerance.
- Gentle grip strengthening using a soft ball or putty to maintain hand function.
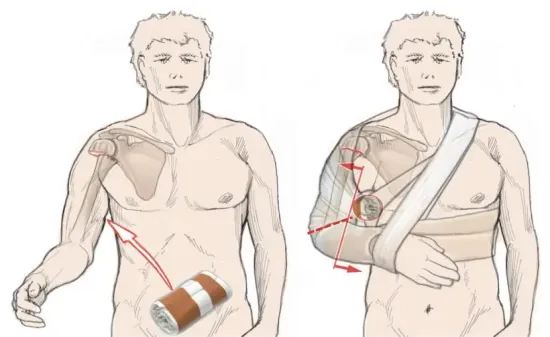
Summary Table: Rehabilitation Protocol for Non-Operative Management of Proximal Humerus Fractures