Achilles tendon rupture is one of the most common lower-leg injuries and can be managed either operatively or conservatively. Not sure if surgery is the best option for an Achilles tendon rupture? Read our full article on this topic:
Operative vs Non-operative Management of Acute Achilles Tendon Rupture.
This Comprehensive Rehabilitation Protocol for Non-Operative Management of Acute Achilles Tendon Rupture outlines an evidence-based, criterion-driven approach to help clinicians and patients navigate safe, structured recovery. It provides clear timelines, functional milestones, and progressions designed to protect tendon healing while restoring strength, mobility, and confidence through every phase of rehab.
Stage 1: Acute Phase (0–2 Weeks)
Goal
- Protect the healing tendon
- Minimize tendon elongation
- Control pain and swelling
- Prevent muscle atrophy and joint stiffness
Interventions
- Immobilize the ankle in maximum passive plantar flexion (equinus position) to approximate tendon ends
- Strict non-weight-bearing with crutches
- Patient education on injury and importance of compliance
Immobilization
- Plaster cast or rigid immobilization in maximum plantar flexion (typically 20°–30° plantar flexion) as per orthopedic team recommendation
- No weight-bearing allowed
Precautions
- No weight-bearing on affected limb
- Avoid dorsiflexion beyond plantar flexed position to prevent tendon elongation
- Monitor for signs of deep vein thrombosis (DVT)
- Educate patient on safe use of crutches and fall prevention
Sample Exercises for Physiotherapists
- Isometric exercises for the knee and hip (e.g., quadriceps sets, straight leg raises) without ankle involvement
- Non-weight-bearing cardiovascular exercises (e.g. Upper Body Ergometer)
- Upper body strengthening exercises
Stage 2: Early Mobilization Phase (2–6 Weeks)
Goal
- Gradual restoration of ankle motion to neutral
- Progressive weight-bearing to stimulate tendon healing
- Maintain cardiovascular fitness and prevent muscle atrophy
- Continue pain and swelling control
Interventions
- Transition from Cast to an Achilles-specific walking boot with heel wedges (usually 40° heel lifts initially)
- Initiate protected partial weight-bearing, progressing by approximately 25% body weight per week (25% at weeks 2–3, 50% at weeks 3–4, 75% at weeks 4–5, 100% at weeks 5–6)
- Begin active plantarflexion and dorsiflexion exercises with dorsiflexion limited to neutral (0°), avoiding dorsiflexion beyond neutral
- Use modalities as needed for pain and swelling (e.g., ultrasound, ice, electrical stimulation)
- Electrical muscle stimulation of calf muscles can be introduced with active heel raises in sitting position
Boot Usage
- Achilles-specific boot with 3 heel wedges maintained
- Gradual reduction of heel wedge height starting around week 6 (one wedge every week)

Precautions
- Avoid passive dorsiflexion beyond neutral (0°) during exercises
- All exercises should be pain-free; reduce activity if pain or swelling increases
- Close monitoring for signs of rerupture or tendon elongation
- Ensure patient compliance with weight-bearing restrictions
Sample Exercises for Physiotherapists
- Active ankle plantarflexion and dorsiflexion to neutral with the boot on
- Toe curls and towel scrunches to maintain foot intrinsic muscle strength
- Seated heel raises with electrical stimulation
- Hip and knee strengthening exercises without ankle involvement
- Non-weight-bearing cardio (e.g., stationary biking with boot on)
- Hydrotherapy as tolerated
Stage 3: Intermediate Strengthening Phase (6–12 Weeks)
Goal
- Achieve full weight-bearing without assistive devices
- Restore ankle range of motion while protecting the tendon
- Begin strengthening calf muscles and improve proprioception
- Prevent tendon elongation and rerupture
Interventions
- Wean off boot gradually over 2–5 days, possibly with night-time use initially
- Remove heel lifts gradually as tolerated, leaving 1–2 lifts to simulate normal shoe heel height
- Initiate resisted ankle plantarflexion exercises using resistance bands or tubing, avoiding dorsiflexion beyond neutral
- Introduce balance and proprioceptive training (e.g., balance board with dorsiflexion blocked)
- Continue modalities for swelling and pain control as needed
Boot Usage
- Gradual weaning off boot (usually by week 8)
- Use of Achilles-specific compression stocking recommended but not mandatory
Precautions
- Avoid dorsiflexion beyond neutral during strengthening and stretching
- Avoid activities that place sudden or excessive load on the tendon (e.g., lunges, squats)
- Monitor for signs of elongation (excessive dorsiflexion compared to contralateral side)
- Educate patient on gradual progression and adherence
Sample Exercises for Physiotherapists
- Active ankle plantarflexion strengthening with resistance bands
- Double heel raises progressing to single heel raises as tolerated
- Balance board exercises with dorsiflexion limitation
- Stationary cycling with low resistance
- Gait retraining focusing on proper heel-to-toe mechanics
- Closed kinetic chain exercises avoiding dorsiflexion past neutral
Stage 4: Advanced Strengthening and Functional Training (12–16 Weeks)
Goal
- Restore strength, power, and endurance of the calf musculature
- Normalize ankle range of motion
- Improve dynamic balance and proprioception
- Prepare for gradual return to functional activities and sports
Interventions
- Initiate calf stretching within safe dorsiflexion limits
- Progress strengthening exercises to weight-bearing closed and open kinetic chain movements
- Initiate low-impact aerobic exercises (e.g., elliptical, treadmill walking)
- Continue proprioceptive training and progress balance challenges
- Avoid high-load activities that cause excessive tendon stretch
Boot Usage
- No boot required
- Use of compression garments may continue for swelling control
Precautions
- Avoid aggressive dorsiflexion exercises
- Avoid high-impact activities, heavy resistance training, running, or jumping
- Monitor for any pain, swelling, or signs of tendon elongation or rerupture
Sample Exercises for Physiotherapists
- Gentle calf stretches
- Weighted heel raises (double and single leg)
- Step-ups and step-downs within pain-free range
- Balance and coordination drills on unstable surfaces
- Low-impact cardiovascular training (stationary bike, elliptical)
- Functional gait training and stair climbing
Stage 5: Return to Sport and Full Activity (16 Weeks to 12 Months)
Goal
- Return to pre-injury activity and sports participation safely
- Achieve at least 80% strength compared to contralateral side before light sports
- Achieve 100% strength before high-impact and cutting sports
- Prevent re-injury and tendon elongation
Interventions
- Gradual introduction of dynamic and sport-specific training (e.g., jogging, skipping, plyometrics)
- Focus on power, endurance, and agility training
- Progressive return to running, cutting, and jumping as tolerated
- Continue strengthening and proprioceptive exercises
Boot Usage
- No boot or heel wedges
- Use of ankle brace or compression stocking optional for support during return to sport

Precautions
- Avoid contact sports and high-intensity activities until adequate strength and control are demonstrated
- Monitor for pain, swelling, or instability
- Emphasize patient education and compliance with gradual progression
Sample Exercises for Physiotherapists
- Progressive running drills starting with straight-line jogging
- Plyometric exercises (hops, bounds) with gradual intensity
- Agility drills (cutting, pivoting) after strength milestones are met
- Sport-specific drills under supervision
- Continued calf strengthening and balance work
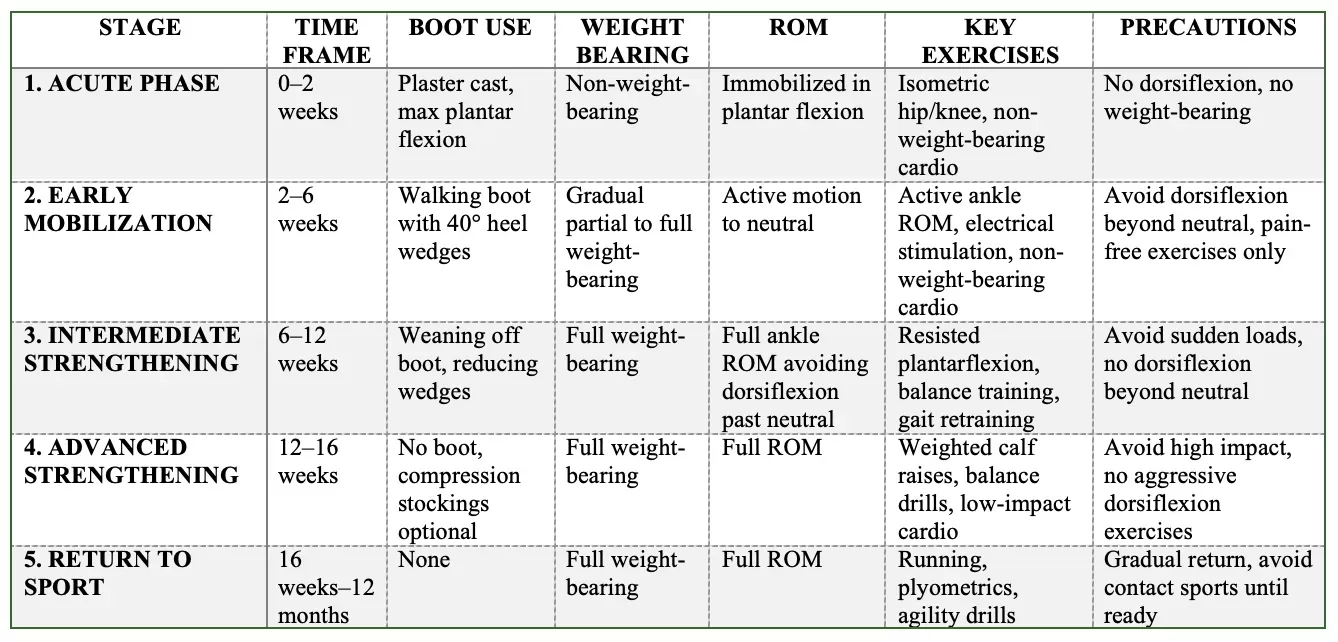
Summary Table of Rehabilitation Stages
Note: Risk of Elongation
Elongation of the Achilles tendon is a potential complication, especially if the rehabilitation protocol is not properly administered or if the patient is noncompliant. It is more likely to occur between 10 to 16 weeks post-injury, as patients regain normal activity. Careful monitoring through physical examination, particularly assessing passive dorsiflexion with the knee extended compared to the contralateral side, is essential to identify elongation early. If elongation is detected, the rehabilitation protocol should be adjusted in consultation with the physiotherapist and physician, potentially reverting to earlier stages of the protocol. In severe cases, surgical shortening may be considered.