Hip arthroscopy has become an increasingly popular, minimally invasive surgical technique to address intra-articular hip pathologies such as femoroacetabular impingement (FAI), labral tears, and chondral injuries, particularly in young and athletic populations. The goal is to reduce pain and restore function, enabling athletes to return to sport safely and effectively.
Femoroacetabular impingement syndrome (FAIS) is a condition characterized by abnormal and dynamic contact between the femoral head–neck junction and the acetabular rim, caused by altered bone morphology such as cam, pincer, or mixed types. This abnormal contact results in progressive damage to the acetabular labrum, chondrolabral junction, and articular cartilage, potentially leading to hip joint degeneration and osteoarthritis. Diagnosis of FAIS is based on a triad of patient symptoms (such as pain, clicking, stiffness, and limited range of motion), specific clinical maneuvers (including the flexion adduction internal rotation and flexion abduction external rotation tests), and imaging studies (orthogonal hip and pelvis X-rays, and MRI or arthrograms). Initial treatment is often conservative, involving physical therapy, intra-articular injections, and activity modification. When conservative management fails or specific criteria are met, surgical treatment, primarily hip arthroscopy, which is a minimally invasive surgical procedure, is performed to correct bony abnormalities and repair or reconstruct labral lesions, aiming to preserve hip function and alleviate symptoms.
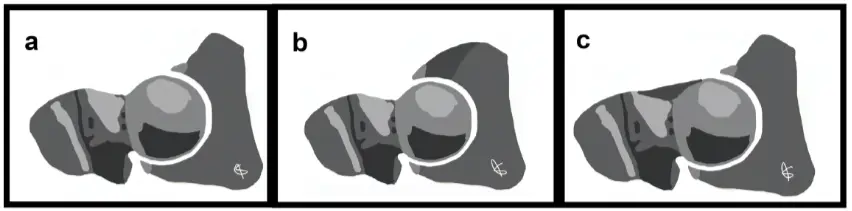
Schematic representation of hip: (a) normal hip, (b) hip with pincer-type impingement (the dark gray zone represents the acetabular over-coverage), and (c) hip with cam-type impingement (the dark gray zone represents the femoral head-neck junction abutment).
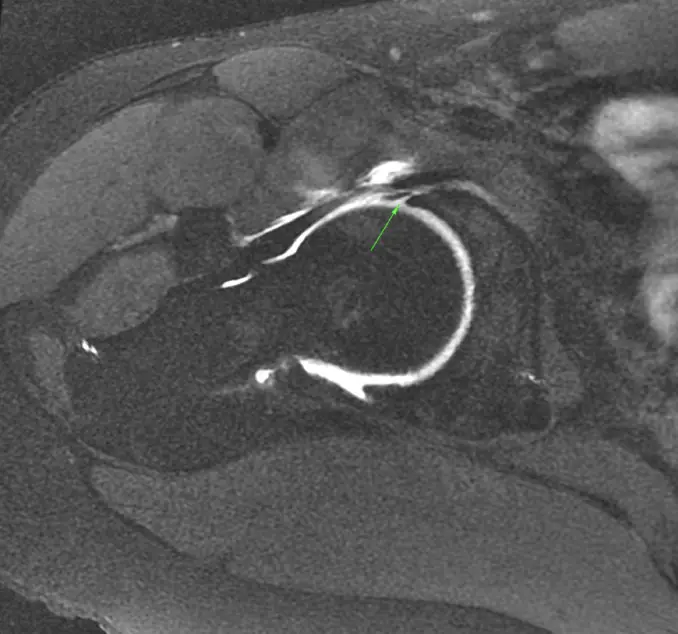
Axial MRA image of a right hip demonstrating a labral tear (arrow)
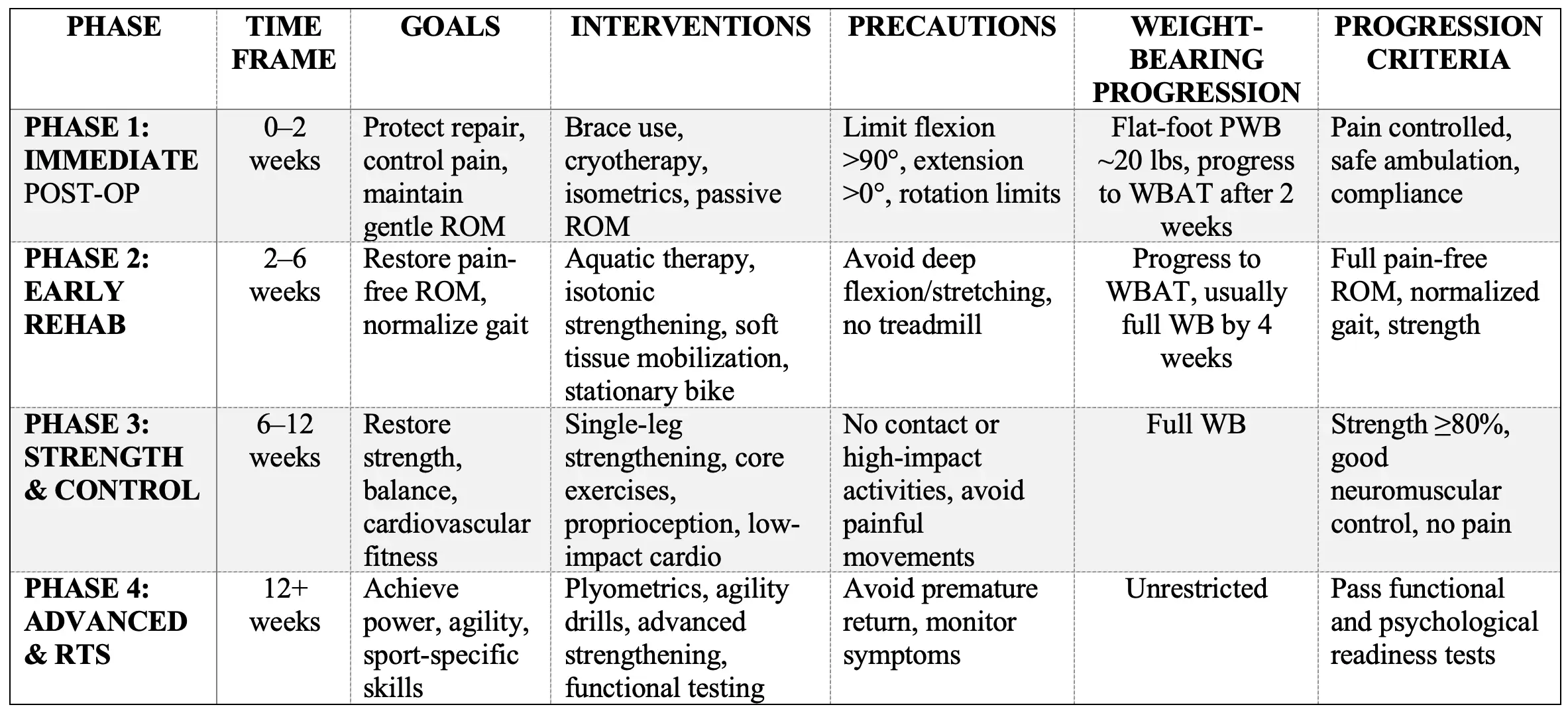
Effective postoperative rehabilitation is crucial to optimize surgical outcomes, restore function, and facilitate a safe return to sport or daily activities. The following protocol synthesizes current evidence and expert consensus on rehabilitation following hip arthroscopy, organized into distinct phases with detailed goals, interventions, precautions, and progression criteria. This comprehensive framework integrates findings from multiple systematic reviews, clinical studies, and expert guidelines.
Summary Table of Rehabilitation Phases After Hip Arthroscopy